The main category of Fitness News.
You can use the search box below to find what you need.
[wd_asp id=1]
The main category of Fitness News.
You can use the search box below to find what you need.
[wd_asp id=1]
Gia Macool is a 1stPhorm Athlete, author, glamour model and public speaker who has been helping people transform their health and fitness since 1998. With over two decades of experience, Gia combines her passion for fitness with her insights from 25 years of marriage to guide others toward stronger bodies, deeper connections, and more fulfilling lives.
Drawing from real-life experience, she shares an honest perspective on what women go through in marriage and the habits that help couples maintain desire, respect, and emotional intimacy over time.
Through her private community, Gia has helped thousands of men and women reach their goals offering practical guidance on personal growth, healthy living, and sustaining long-term relationships.
She also partners with international and local brands and has been featured on magazine covers and media platforms around the world.
Women Fitness President Ms. Namita Nayyar catches up with an exceptionally talented and accomplished, Gia Macool who is a 1stPhorm Athlete, author, glamour model and public speaker. Here she talks about her fitness regime, diet and success story.
You’ve been a prominent figure in the health and fitness world since 1998. How have the industry—and your role within it—evolved over the years?
I’ve transitioned from competing to living a balanced fitness lifestyle. What first led me to fitness—a passion for health and quality of life—hasn’t changed. With experience come wisdom and the ability to handle challenges at every level, whether competitive or personal.
Now, I focus on helping everyday women—wives and mothers—get fit and feel their best. The industry itself has also shifted to a more mainstream focus on wellness.
You wear many hats: 1st Phorm Athlete, author, model, and relationship guide. How do these roles come together in your mission?
All of these roles connect through one purpose—wellness. It’s about creating a long, fulfilling life and becoming the best version of yourself.
Relationships are key to every area—fitness, business, or family. The way you treat people and maintain those relationships ultimately defines your success.

The term “glamour model” often carries preconceptions. How have you used that platform to promote health and empowerment?
Glamour modeling often gets misunderstood because many in the industry drift from beauty into exploitation. Women are told that doing “more” means making more money—but that usually comes with a cost.
I aim to help women model in a healthy, confident, and value-driven way, maintaining boundaries while building real relationships and staying mainstream.
As a 1st Phorm Athlete, what about their philosophy and products aligns with your own?
1st Phorm holds a high standard—not just in their products, but in their people. They always go beyond what’s promised, which is exactly how I approach my work: under-promise, over-deliver.
What’s the biggest mental or emotional hurdle that holds women back from starting their fitness journey—and how can they overcome it?
Comfort.
Most women stay stuck in what feels safe. But growth happens in discomfort. Stepping out of that zone builds strength, not just physically—but mentally too.
Full Interview is Continued on Next Page
This interview is exclusive and taken by Namita Nayyar, President of womenfitness.net, and should not be reproduced, copied, or hosted in part or in full anywhere without express permission.
All Written Content Copyright © 2025 Women Fitness
Disclaimer
The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
By Linzi Martinez, CPT, INHC, BA
The fitness world is entering a breakthrough era. If the last few years were about “just move more,” 2026 is about precision, personalization, and intelligent support meeting you exactly where you are, and evolving with you as your body, lifestyle, hormones, and goals shift. The days of generic programs are fading fast. Today’s apps are smarter, more intuitive, more biologically informed, and more capable of delivering actual results than ever before.
A powerful combination of AI innovation, wearable integration, human expertise, and a growing understanding that fitness is no longer about workouts alone. It’s about whole-person health…sleep, stress, hormones, metabolism, mindset, and daily accountability…finally coming together in one ecosystem.
And for the first time, the technology has caught up.

2026 is shaping up to be the year that fitness apps move from being simple tools to becoming full-fledged wellness partners, supporting everything from strength training and metabolic health to stress management, gut function, and hormonal balance. The level of innovation, intelligence, and accessibility is extraordinary and the industry is recognizing it in a big way.
From free apps making high-quality training accessible to everyone, to mid-tier AI platforms delivering adaptive programs, to elite concierge services offering white-glove care with real human experts, this year’s lineup reflects one of the most exciting evolutions the fitness world has ever seen.
Below are the apps poised to dominate 2026—three in each category; each offering something powerful, unique, and perfectly aligned with the future of wellness.
These apps are perfect if you’re self-motivated and want world-class workouts, expert guidance, and plenty of structure—without spending a dime. What makes 2026 so exciting is how high-end these free platforms have become.

NTC continues to dominate the free-fitness world with one of the most comprehensive workout libraries anywhere online. Nike Members now get unlimited access to 190+ free workouts across strength, endurance, yoga, mobility, Pilates, recovery, and even mindset training. The interface feels premium, the production quality is exceptional, and the level of coaching rivals paid programs. This year, Nike added more structured programs, progression-based plans, and specialty series for mobility, athletes, and beginners …making it a true all-in-one platform for anyone seeking professional-quality workouts without cost.
Women who want high-quality, structured training without the price tag.

FitOn exploded in popularity because it brings together the feel of boutique studio classes like Pilates, yoga, HIIT, strength, dance cardio with the accessibility of a free app. In 2026, FitOn continues expanding its offerings into stress management and recovery, integrating meditations, breathing sessions, and stretching flows that support women dealing with burnout, anxiety, or hormonal stress. Its celebrity-led classes and community-driven energy make working out feel fun, uplifting, and achievable.
Women who crave variety, energy, community, and stress relief while keeping fitness fun and free.

Samsung’s partnership with iFIT has created one of the most seamless, integrated fitness experiences available. Users can access monthly free guided workouts including strength, yoga, Pilates, core, recovery, walking, and barre directly inside Samsung Health. Automatic syncing with Galaxy watches creates a unified, user-friendly wellness dashboard.
Women who want smart, integrated tracking and a polished fitness experience.
Disclaimer
The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
You’ve probably seen the hepatitis B vaccine in the news lately.
If you’re wondering what the buzz is about, let’s start with the basics.
Hepatitis B is a liver infection caused by the hepatitis B virus (HBV). The infection can be short-term or last for life, and it can cause severe complications such as liver failure, liver cancer and even death.
“Hepatitis B is a dangerous infection — it can be life-threatening for a person of any age who contracts it,” said Deborah L. Wexler, M.D., founder and executive director emerita of the Immunization Action Coalition.
The hepatitis B virus is highly contagious, so it spreads very easily through body fluids. Even sharing a toothbrush can transmit HBV. And the virus can also live on surfaces for days.
About half of people with hepatitis B don’t have symptoms, which means they can pass on the virus without even knowing they have it.
The great news is that hepatitis B is preventable, thanks to the vaccine. Since 1991, the recommendation has been to give the first of three doses of the hepatitis B vaccine to all newborns at birth. After the recommendation was implemented, hepatitis B infections in children decreased by 99%.
This is where the latest news comes in: Earlier this month, the CDC’s Advisory Committee on Immunization Practices (ACIP) voted to withdraw the recommendation to vaccinate every newborn for hepatitis B at birth (called the “universal birth dose”) and now recommends the birth dose only for newborns whose mothers test positive for the virus. For other newborns, ACIP now recommends that they should get the first dose of the vaccine “no earlier than two months of age.”
Wexler, who has spent much of her career helping implement the birth dose in the U.S., said rolling back the universal birth dose recommendation is dangerous for a few reasons.
For one, many pregnant people aren’t tested for hepatitis B, which puts their newborns at risk during childbirth.
When newborns and children up to 5 are infected, they often become lifelong carriers of the virus and are more likely to have serious health problems.
The best way to prevent hepatitis B infection is by getting vaccinated.
Here are 4 things you need to know about the hepatitis B vaccine.
Most people have life-long immunity after getting the hepatitis B vaccine. But you have to get all the doses for full protection.
The number of shots and the amount of time you have to wait between doses varies depending on the vaccine.
Decades of research have shown that the vaccine is safe and effective in protecting against hepatitis B and that side effects, if any, are mild.
Hepatitis B is spread through contact with infected body fluids (saliva, vaginal fluids, semen, blood).
Most people are exposed to the virus through:
But you can also contract hepatitis B off of infected surfaces. The vaccine protects against all types of exposure to the virus.
Waiting two months to give the hepatitis B vaccine opens up a two-month window for babies to get the virus when their immune systems are young and vulnerable. In addition, not all pregnant people are tested for active or chronic hepatitis B. In fact, in the U.S., an estimated 500,000 pregnant women are not tested each year, so their status is unknown at the time of delivery.
Wexler said the vaccine is a matter of public safety and helps you and your loved ones — and really everyone — live free from chronic liver disease.
“[Without the universal birth dose], a lot of those babies will fall through the cracks. If there’s no hepatitis B result on the chart and they’re not vaccinated, then those children are at severe risk for hepatitis B from their mothers. So the universal birth dose is a safety net — and safety nets are what public health is about. We have the opportunity to eliminate hepatitis B from the United States — and from all over the world — by utilizing this vaccine,” Wexler said.
From Your Site Articles
Related Articles Around the Web
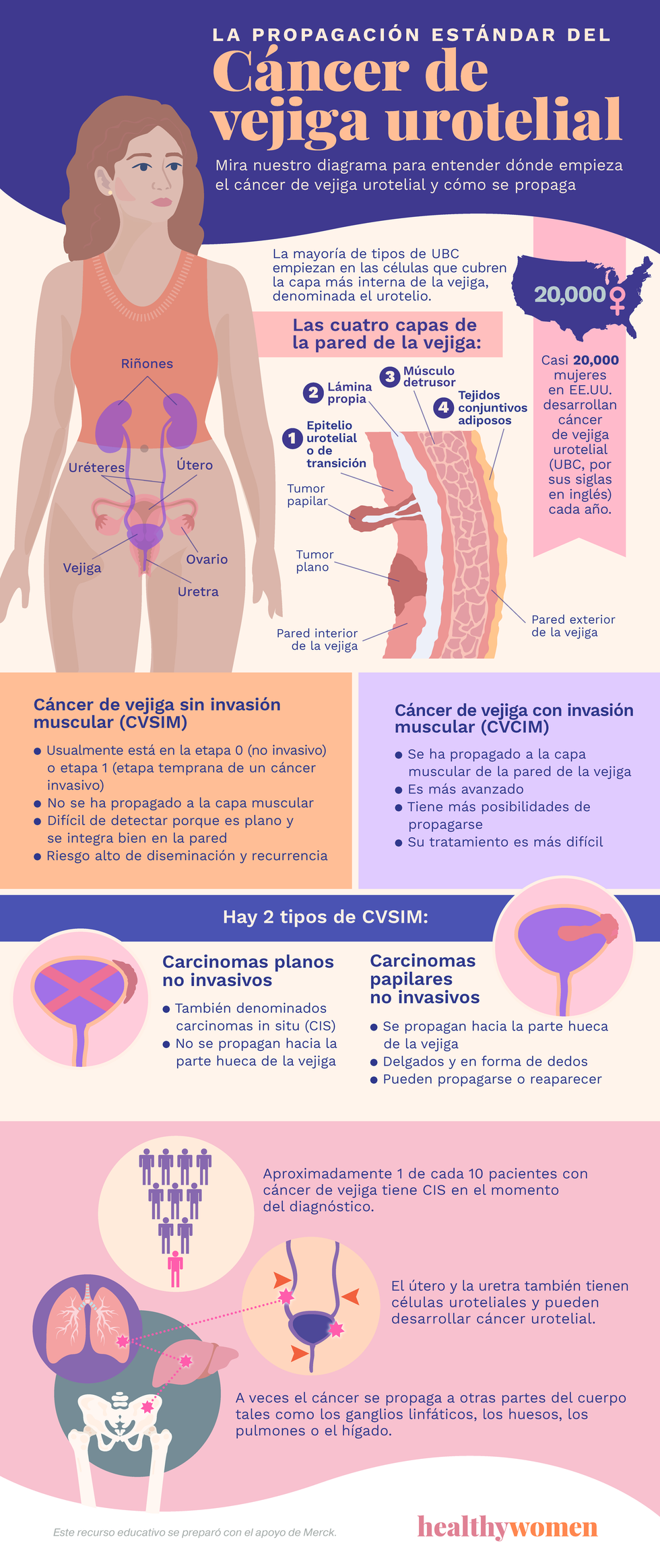
Casi 20,000 mujeres en EE.UU. desarrollan cáncer de vejiga urotelial (UBC, por sus siglas en inglés) cada año.
Las cuatro capas de la pared de la vejiga:
Epitelio urotelial o de transición
Lámina propia
Músculo detrusor
Tejidos conjuntivos adiposos
La mayoría de tipos de UBC empiezan en las células que cubren la capa más interna de la vejiga, denominada el urotelio.
Cáncer de vejiga con invasión muscular (CVCIM)
Cáncer de vejiga sin invasión muscular (CVSIM)
Hay 2 tipos de CVSIM:
Carcinomas planos no invasivos
Carcinomas papilares no invasivos
Aproximadamente 1 de cada 10 pacientes con cáncer de vejiga presentan CIS en el momento del diagnóstico.
El útero y la uretra también tienen células uroteliales y pueden desarrollar cáncer urotelial.
A veces el cáncer se propaga a otras partes del cuerpo tales como los ganglios linfáticos, los huesos, los pulmones o el hígado.
Este recurso educativo se preparó con el apoyo de Merck.
Brittany Barreto, Ph.D., is a podcaster, an entrepreneur, and a molecular and human geneticist. (In other words, she’s really smart.) Read her column here each month to learn about what’s happening in the world of technology and innovation in women’s health.
Painful periods can be more than an inconvenience. Menstrual pain, officially called dysmenorrhea, affects up to 9 out 10 people who menstruate at some point in their lives. But, for 5% to 10% of women, cramps can be so intense that they interfere with work, school or daily life.
Traditional treatments like over-the-counter pain medication or heating pads don’t work for everyone. But thanks to advances in wearable and neuromodulation technology, new tools are offering drug-free ways to manage menstrual pain and even help some users reduce heavy flow and fatigue.
Here’s a look at four emerging devices designed to interrupt menstrual pain signals: Livia, OhmBody, Jovi and Samphire.
Livia: Turning menstrual pain “off” with micro-pulses
(Photo/Courtesy of Livia)
Livia is a compact wearable FDA-cleared device that uses patented SmartWave micro-pulse technology to block pain signals before they reach the brain. Worn discreetly under clothing, the device delivers gentle electrical pulses to the lower abdomen.
This approach, based on the gate control theory of pain,reduces pain perception and stimulates endorphin release. Relief can begin within 30 to 60 seconds of turning it on.
Several double-blind, randomized clinical studies have shown that Livia significantly reduces pain in people with primary dysmenorrhea (period pain without an underlying condition). Livia is FDA-cleared, Health Canada-approved and CE marked for use in the European Union.
The device is sold online and through major U.S. retailers like CVS. However, it’s not currently covered by insurance, meaning users must pay for the device out of pocket.
OhmBody: A brain-based approach to lighter, calmer cycles
OhmBody takes a different route than Livia, targeting the vagus and trigeminal nerves through small earpieces rather than the abdomen. These nerves help regulate the body’s “rest-and-digest” versus “fight-or-flight” response, which can be helpful during menstruation, when the nervous system often shifts into stress mode. OhmBody’s gentle neurostimulation aims to help with pain, reduce blood loss and improve mood.
OhmBody has been clinically tested for safety. The peer-reviewed study was conducted by Spark Biomedical, OhmBody’s parent company, and it was very small — but the early results were promising. In this pilot trial of 16 participants, use of the wearable neurostimulation device was associated with a reduction in menstrual blood loss, shorter periods, and improvements in pain and quality-of-life scores.
While these findings are encouraging, it’s important to note that OhmBody is currently marketed as a wellness device, not a medical treatment. That means it’s not FDA-cleared for menstrual pain and is not covered by insurance. If you want to use OhmBody, you must purchase it directly from the company and pay for it out of pocket. You may be able to use funds from your HSA or FSA account to buy OhmBody, but you’ll have to check your plan rules to find out.
Jovi: A reusable patch without electricity
Jovi looks like a flexible sticker, but it uses a unique signal-filtering technology made from microscopic conductive particles to reduce pain. Unlike OhmBody and Livia, instead of sending pulses into the body, Jovi claims to “absorb and reroute” pain signals, similar to tuning out static on a radio.
Jovi patches can be worn anywhere on the body and are reusable for up to a year. They’re drug-free and water-resistant. As wellness devices, they are not FDA-cleared, but they are eligible for HSA/FSA purchases. While Jovi’s approach is different from electrical or heat-based devices, it’s still an emerging technology. Early customer feedback has been positive, and many users report noticeable relief, though additional independent research would help confirm its effectiveness. Jovi is available online in the U.S. and prices start at $159 per patch.
Samphire: Menstrual care that starts in the brain

(Photo/ Courtesy of Samphire)
Samphire Neuroscience is a London-based company pioneering brain-based approaches to menstrual health, addressing both menstrual cramps and hormone-influenced mood shifts. Its first product, Nettle, is a CE-certified medical device (meaning it has met rigorous health, safety and environmental requirements in the EU) intended to help manage pain and mood changes related to PMS, premenstrual dysphoric disorder (PMDD) and endometriosis. Nettle is currently available only in the EU and the UK.
Samphire’s upcoming U.S. device, Lutea, uses similar non-invasive brain stimulation (tDCS), a gentle, low-level electrical current applied through electrodes on the scalp. Clinical studies show that tDCS can safely modulate brain activity linked to mood and pain perception.
Lutea is marketed as a wellness device, meaning it doesn’t make medical claims and is not yet FDA-approved. The company expects to pursue approval as research expands. In fact, Samphire is actively recruiting participants to study their product’s ability to modulate pain and emotional regulation in patients with endometriosis in London and California. Preorders for U.S. buyers are open, but insurance coverage is not available — and the price is steep, starting at $589.
From pain to progress
For decades, women have had limited, often unsatisfying options for menstrual pain relief. Now, a wave of wearable and brain-based technologies is offering new hope and proof that women’s health innovation is finally catching up.
Still, most of these devices are not yet covered by insurance and are not intended to replace medical care. Anyone with severe pain, heavy bleeding or conditions like endometriosis or fibroids should talk with a healthcare provider before using new devices.
These tools represent an important shift, one that moves menstrual pain from something women are expected to tough out to something science can actually solve.
The information about products and/or services in this column does not constitute any form of endorsement or recommendation by HealthyWomen. Links are provided as a convenience and for informational purposes only. This column may occasionally cover companies in which Brittany Barreto is an investor.
From Your Site Articles
Related Articles Around the Web
Think back to 1993. What do you remember?
Seeing the movie Jurassic Park on the big screen? Listening to Whitney Houston’s “I Will Always Love You” on the radio? Surfing the World Wide Web for the first time?
1993 was also the year the government began requiring that the National Institutes of Health include women in medical research.
Yep, you heard that right. It was just 32 years ago that the NIH Revitalization Act passed mandating that women be included in clinical studies and other research.
The landmark bill was a huge step forward, propelled by women’s health advocates. But still to this day, only 8% to 11% of the NIH grants currently fund women’s health.
This detail was not lost on Liz Powell. After working as an attorney, lobbying in Congress for 25 years and running a bipartisan firm, G2G Consulting, she started Women’s Health Advocates (WHA) in 2024. WHA is a bipartisan coalition with a mission to help shape the legislative process, educate government decision-makers on women’s health and secure funding for advancements in women’s health.
We talked with Powell and Elizabeth Garner, M.D., MPH, a founding member of WHA, about the organization’s first year and how they’re keeping the spotlight on women’s health.
This interview has been lightly edited for clarity and length.
HealthyWomen: Liz, can we go back to the beginning and talk about why you started Women’s Health Advocates?
Liz: I’ve done a lot in the health space and try to bring life science innovations to market by working with the government to accelerate access to government funding.
I would have a couple clients here and there that were touching on the woman’s health space. Every time you get a new client, you learn about different gaps where unmet needs need solutions. I realized this is not just a one off here and there — there’s a real pattern going on. So I helped organize these two new coalitions and efforts to do better advocacy and education on women’s health and realized we needed something as the umbrella for all of it. And that’s what Women’s Health Advocates is.
We launched in February of this year. But like I said, it’s the culmination of work of many of us, including doctors — Dr. Garner has been a huge advocate in women’s health — and there have been many, many people working really hard in the women’s health space for a long time.
What Women’s Health Advocates is trying to do is bring all that together for advocacy, all aspects of the ecosystem. So, whether you’re a researcher or clinician, CEO, entrepreneur, investor, patient — no matter where you are in this ecosystem, there’s a place for you at Women’s Health Advocates.
We want to change laws, we want to increase funding, work with the government and make sure politicians understand the impact their decisions have on the health of women.
HealthyWomen: Dr. Garner, what was it about WHA that made you want to get involved?
Elizabeth Garner: Most of it was that I really like Liz (laughs). We’ve known each other for a while.
Everything she said is what I was thinking — and going through. First, as a women’s health physician, I was frustrated by the lack of solutions for so many conditions like endometriosis and polycystic ovary syndrome (PCOS) and fibroids, and you can just keep going on and on.
I saw women just really suffering — and their families. I felt like we just needed so much more. And then I left clinical medicine because I was hoping if I got into industry, maybe I’d have a bigger impact. And unfortunately what I found was that we don’t have the solutions I wanted as a physician because there just hasn’t been the research.
Modern medicine was really developed for male physiology, and it was assumed that women were small men. Because of that, we don’t actually understand the fundamental science that’s underlying all of these conditions. And that hurts from a therapeutic standpoint but also from a diagnostic standpoint. So we don’t actually have good ways even to diagnose a lot of the conditions I’ve mentioned . Women go years before they know what’s wrong. We still don’t know why women are different from men in many ways.
That’s still going on and there’s been a lack of innovation, investment, etc in women’s health. That’s really why we want to bring anyone, everyone into this organization — meaning not just women but men. We have a lot of male supporters, but in terms of history, men have been the deciders of where dollars go when it comes to health, so over time, women’s issues haven’t been considered to be as important as men’s issues. By bringing this whole ecosystem together, we can really make a difference. And that’s why I joined.
HealthyWomen: Tell us more about the needs WHA addresses and anything noteworthy you’d like to spotlight.
Liz: I would say — putting on my lobbying hat — to be an effective lobbyist, to have tangible results, I want to jump onto a train that’s already moving. I want to do general education advocacy about the long-term gains that we need in women’s health. Well, that train is called appropriations.
Every year, the House and Senate have to do these appropriations bills. That, plus the National Defense Authorization Act, gets done every year no matter what. The appropriations is where we put a lot of focus, we lobbied our tails off and we got in there to get language and funding lines included in the appropriations bills, and we’re actually seeing results. Our success was a combination of my lobbying team, which is me and my folks at G2G Consulting, as well as the letter writing campaign.
We would draft letters for folks and got our grassroots advocates who are in all 50 states writing letters. We also organize Capitol Hill events, and we had our first event in April focused on Centers for Medicare and Medicaid Services (CMS) reimbursement discrimination because, on average, the same surgery performed on a female and a male patient has a 30% lower reimbursement rate if it’s a female patient.
Doing a congressional briefing opened a lot of eyes. A lot of people started to ask questions and want to work with us, so that’s great.
On May 21, we did the first-ever women’s health Capitol Hill Day where we addressed all of women’s health with great bipartisan turnout from members of Congress.
In July, we had our breast cancer Hill day. Every time we do these, we’re bringing advocates to Washington to share their stories to shape the legislative process. And the results that we’re seeing all came out in the summertime and showed that the language we had lobbied for, like the definition of woman’s health, which is conditions that solely, disproportionately and/or differently impact the health of women, head to toe throughout their lifespan, is actually in the bill on the house side.
Our funding request for a $30 million increase for the Office of Research on Women’s Health has been included in the Senate bill and in the House bill; it’s a $26 million increase. So, either way, that office is going to get an increase.
So, all those efforts are really producing results. We’ve still got a ways to go, but at least we’re seeing something in less than a year.
Garner: Liz is the policy wonk. I am so not and I’m learning, but just from my perspective, another thing I think that WHA is clearly doing is raising awareness.
As we go around the country, more and more folks are coming in and it’s amazing — because we know this stuff, but most people don’t. So, we talk about data around lack of innovation and NIH funding and all of that and venture capital funding. We’re doing a lot of education as well, and that’s really important and will help us as we continue to talk about policy.
HealthyWomen: What are the group’s goals for 2026?
Liz: We are heading into an election year, so that will be a big factor. Because we are not a nonprofit, we can engage in politics as much as policy.
We are going to be tracking what’s going on on the policy front. We’ll be doing more appropriations work next year. And then we’ll also be tracking the candidate, and candidates that are in what are called “persuadable districts,” where the person wins by anywhere from 1% to 5%. Those are persuadable districts that could flip either way. And that’s where there’s the most power in shifting and making women top of priority. So, we’ll focus on those — we’ll track those.
We really want to do a whole get out and vote for women’s health campaign. We’re already working with Beyond the Paper Gown on doing a whole series to educate people on women’s health issues and why it’s important to go out and vote.
Garner: I think the awareness part, as I was mentioning, is going to be really important but also homing in on our strategy going forward is going to be really important to keep moving forward.
HealthyWomen: How do supporting organizations like the Society for Women’s Health Research and HealthyWomen play an important role in advancing these goals?
Liz: It’s critical. The Society for Women’s Health Research is doing lots of great advocacy work, but they are nonprofit so they are limited in how much they can do. And so a lot of times that we team up when they’re working on something and we can amplify it.
We’ve signed on to letters that they sent to Congress, for example, and we’ve written letters that they’ve signed on to. There’s a lot of very supportive partnership and collaboration that happens.
Garner: There’s just no one organization that can do this alone. And so we talk a lot about bringing together the entire ecosystem so everyone is working together.
HealthyWomen and SWHR provide women with information and safe spaces for women to tell their stories. And that’s what drives people. That’s what drives policymakers, investors and other stakeholders to take action when they hear those stories.
HealthyWomen: How can readers get involved?
Garner: We’re doing events around the country, so we definitely invite people to come to an event and see what’s happening and learn and meet like-minded people.
Liz: People can also sign up on our website to join our community — I send legislative updates and a lot of insider information most people don’t have with women’s health always being the focus.
HealthyWomen: Is there anything else you’d like to add that we haven’t talked about?
Garner: I have one thing that I think it’s always important to talk about, and that’s diversity. We are a very diverse organization. And it’s so important because, for all the issues that we’ve been talking about, they are always worse for women of color, for other underserved communities and so on. So, we’ve got to make sure that, as we go along, we’re including everyone in all that we do.
Medically reviewed by Armine Smith, M.D.
Let’s face it, the holiday season always delivers a contradictory blend of magic, wonder and overwhelm, and a pair of slipper socks may not take the edge off your laundry list of to-dos.
Finding time to relax and recalibrate before the decorations are packed away may seem impossible, but the better you treat yourself, the more you can inhale happiness and exhale burnout.
We’ve created a list (and checked it twice) of 12 ways to practice self-care during the holiday countdown. From mini indulgences to healing experiences, prioritizing self-care every day, no matter how small, will keep you present and balanced and help you manage festivity overload.
A session with a Reiki practitioner or using a sound healing app can help clear emotional blocks, alleviate stress and fill your tank.
International Association of Reiki Professionals, Soaak
Instead, mindfulness and manifesting journals focus on the big picture and are designed to help you reflect on your goals and overall well-being. Light a candle, pick up your favorite pen and set your dreams in motion.
The Growth Guided Journal, The Human Being Journal
What would it be like to have a stylist dress you during the holiday season? If this sounds like a dream but out of your price range, we have good news. Online personal styling services like Stitch Fix take the guesswork out of holiday dressing, have no fees and don’t require a subscription.
Sleeping in total darkness, disconnecting from digital devices and feeling comfortable in bed can help you reach your sleep goals.
Accuratex Cooling Sheets, Blissy Sleep Mask, Reacher Sunrise Alarm Clock
Read: Top 8 Healthy Sleep Habits >>
Staying local? A new makeup bag for trips to the office or the gym feels like a fresh start without the broken zippers and exploded eyeshadow stains.
Lola Makeup Bag, Terra Hanging Toiletry Bag, The Foldie Toiletry Bag
Latte lover? Grab some holiday creamers or a frother for a barista-worthy coffee you can make on the fly and enjoy anytime. Pair it with a short visual meditation for a fully relaxing coffee break.
Bodum Pour Over Coffee Maker, Instant Pot 4-in-1 Milk Frother, Milk Frothing Thermometer
Read: Hot Stats on Warm Bevvies: Can Hot Beverages Help with Healthy Aging? >>
Take your time, sketch or write in a notepad, or simply sit for a while and enjoy the view. And, if you want, you can pick up some stocking stuffers at the gift shop, crossing one item off your to-do list.
Kyrgies Wool Slippers, Organic Turkish Waffle Robe, UNIQLO Wide Sweatpants
Meet up for coffee, hop on a Zoom call with a remote bestie or invite your crew over for a girl’s night in: DoorDash, fuzzy socks and spa masks are mandatory.
Celestron NexYZ, Monocular Telescope for Smartphone, Night Sky App
From Your Site Articles
Related Articles Around the Web
There was a taste of fall in the air. The musty scent of leaves hung heavy as they crunched beneath our feet. October days were getting shorter. And the holidays were looming like shadows in the late afternoon sun. I regarded the soon-to-be festive season with an unsettling feeling of impending doom.
This was an autumn like no other. My husband Joe and I were headed to my outpatient physical therapy appointment. My legs were stick thin and I walked like a newborn fawn on wobbly, unsteady limbs. My weight had dropped to 115, and my hair was falling out. I lived an anxiety-riddled existence. Crying every day and waking up in a panic after a fitful sleep filled with horrendous nightmares.
Five months earlier, on May 22, 2021, my colon perforated from undiagnosed diverticulitis, a serious infection. I went into septic shock, my immune system’s dysfunctional way of fighting the infection, and my organs started to fail. Our world was rocked in an instant as I was flown by helicopter to shock trauma for emergency surgery in Baltimore. The doctors were doubtful I’d make it.
Surprisingly, I did. A large part of my colon was removed, and a temporary colostomy was placed by pulling a small piece of intestine through my abdominal wall to create a stoma to get rid of waste while my intestines healed. My colorectal surgeon, a brilliant physician with skillful hands, said she would reconnect everything by doing a colostomy reversal in December. The nurses marveled over my neatly stapled 10-inch incision that ran straight down my stomach and through my belly button. They said the stoma was “beautiful.” My surgeon had done amazing work, but I wasn’t sure about calling the stoma “beautiful.”
Jackie in shock trauma ICU after suffering from septic shock, 2021.
I spent over a month in the hospital and inpatient rehab. Only to be re-admitted again to drain a post-op infection shortly after I came home. I had to learn to walk again and brush my teeth. I had to adapt to the stoma. Sepsis left me drained and my muscles wasted away. I couldn’t pour a bowl of cereal and could barely sit up for more than 10 minutes at a time.
My nerves were shot. My family did everything they could to ease my mind, but they didn’t understand what was happening. I didn’t even realize I was suffering from PTSD and post-sepsis syndrome, a condition that affects about 50% of survivors, but no one knows much about. We suffer in silence. My mind had been overtaken by irrational fears of just about everything. I was terrified to have bloodwork done or my vitals taken. I started to emotionally detach from life itself. I was tuning out, just like the blank screen on the TV that I would stare at for hours.
The holidays, and my next surgery, were fast approaching. I was so sure that I wouldn’t survive the reversal that I booked the surgery for December 8to be sure I didn’t miss my youngest daughter Alexis’s 21st birthday on the 5th. I wanted Alexis to enjoy that milestone, just in case I didn’t make it.
Alexis, my other daughter Elise, and my son Joey and his fiancé Colleen, assured me they would handle the holidays. Meanwhile, I had a calendar full of “must-dos.” A colonoscopy, to check if everything was okay inside for surgery. Iron infusions, tons of bloodwork, cardiology clearances, pulmonology clearances and a physical. This surgery was no walk in the park. It would take several hours and was very complex. I also have several chronic, disabling conditions, including Hypermobile Ehlers-Danlos, POTS, Crohn’s disease and severe osteoporosis. I had a lot of pre-surgery boxes to check.
Come November, my husband suggested we go to a nearby lake and take walks as the afternoon sun was getting even lower in the sky. The leaves were really rustling now. The walks helped settle my mind a bit and strengthened my muscles for surgery. I continued with outpatient physical therapy. I was still very weak — and plagued by my mental demons of doom.
Thanksgiving arrived on a bright sunny November morning. Elise and Alexis helped their dad get everything ready. They made all the things — turkey, stuffing, potatoes and pie. Joey and Colleen brought more food and cookies. New memories were forming around me, just as savory as the meal. As we sat around the table, and the kids joked and laughed, I looked around intently and tried to take a mental snapshot and put the picture away in my heart. Just in case my fears came true.
Before Alexis left that weekend to go back to college, I gave her an early birthday present. A Pandora bracelet and a 21 charm, with her birthstone. Tears welled up in my eyes. I was convinced I’d never live to see her graduate, much less see her return home for Christmas break in a few weeks. I tried not to give away my fears, but I failed miserably.
 Jackie and Alexis with Alexis’ 21st birthday charm bracelet, 2021
Jackie and Alexis with Alexis’ 21st birthday charm bracelet, 2021
December rolled in with a crisp chill. I avoided listening to Christmas music. It was too wistful and sentimental, and it hurt my heart and a huge lump formed in my throat. Bing Crosby’s “You’re all I want for Christmas,” has always been a sore spot. My dad used to play it on the family stereo when I was little, and it makes me think of family who are no longer here. And now, I worried that it would be the last time I’d be here to hear holiday songs. Instead, I kept smooth jazz on the radio. Nice, neutral territory.
My nerves were fraught with tension and terror the morning of my surgery check-in at 5 a.m. in Baltimore at the same hospital. I almost escaped and ran out the front doors. My husband coaxed me back inside, and a registration staff member named Tatia came over and sat with me and held my hands. She gently prodded and asked what was wrong. I told her I was sure I was going to die in surgery. Tatia asked me about my kids, their careers and what had brought me there that morning. I gushed about my kids and then told her about the sepsis and my previous flirtation with death. She assured me I was very strong to have survived that, and I would survive this too. She came upstairs with us to the pre-op area and stayed until my surgeon arrived. It was like I had an angel looking out for me that morning.
When I woke up in the recovery room, the nurses gleefully announced that I had made it. I was on the other side! Just not “that” side. I was still on this planet, much to my surprise. I peeked under the covers at the small white bandage on the left side of my stomach where my stoma used to be. My surgeon said the takedown was a success, although it took a few days for everything to start working again. I spent eight days in the hospital, walking in the halls dragging my IV pole. Joe filmed my progress for Instagram. One of my nurses fashioned a makeshift sparkly pipe cleaner into a Christmas ornament and attached it to my IV pole. It was the most beautiful decoration I’d ever seen.
 Jackie and her kids, Christmas 2021
Jackie and her kids, Christmas 2021
The day after I came home, our son drove to Pittsburgh to bring Alexis home for break. The girls had insisted on waiting till I came home to decorate the tree. I was still frail and weak. But I was able to lie on the couch and watch them hang ornaments while playing the Christmas song guessing game with their dad. Alexis put on classic Christmas carols (the really old ones), and when the first few seconds of the song began, she’d ask her dad to name the artist. They had played this game for years.
My husband helped make a few purchases online, so we’d have something for the kids on Christmas morning. Elise had purchased a Fitbit way back in September so I could keep track of my steps as I continued my recovery. She always was more certain of my survival than I was. Joey and Colleen bought me a Wii Fit so I could workout at home on my off days from physical therapy. Alexis made the best meal, and it felt like we opened a new chapter. Waves of emotion erupted as I opened the gifts. I really didn’t need the gifts; my family was all I needed. It felt surreal. To still be alive. Like a dream. Our Christmas dream. And it was all I ever wanted that Christmas.
Resources
Have your own Real Women, Real Stories you want to share? Let us know.
Our Real Women, Real Stories are the authentic experiences of real-life women. The views, opinions and experiences shared in these stories are not endorsed by HealthyWomen and do not necessarily reflect the official policy or position of HealthyWomen.
From Your Site Articles
Related Articles Around the Web
Celia Quansah is an English rugby sevens player who plays for Leicester Tigers Women. She was selected as a member of the Great Britain women’s national rugby sevens team for the 2020 Summer Olympics. Born at Twickenham, England. Born to a Ghanaian father and English mother, Quansah grew up in Twickenham. She participated in athletics, winning the long jump event at the 2011 School Games, and represented England internationally in heptathlon, competing at the British Championships against Jessica Ennis-Hill. Whilst at university, she took up rugby. After playing for six months, she was invited to join the England Sevens programme for 2018/19, and played for the winning Great Britain team at the 2019 Rugby Europe Women’s Sevens Olympic Qualifying Tournament.
She was selected as a member of the Great Britain women’s national rugby sevens team for the 2020 Summer Olympics. She was named in the England squad for the 2022 Rugby World Cup Sevens – Women’s tournament held in Cape Town, South Africa in September 2022.
Women Fitness President Ms. Namita Nayyar catches up with Celia Quansah – an exceptionally talented and accomplished English rugby sevens Olympic athlete. Here she talks about her fitness journey and the success story.
You were born in Twickenham, England. You participated in athletics, winning the long jump event at the 2011 School Games, and represented England internationally in heptathlon. While at university, took up rugby and after playing for six months, were invited to join the England Sevens programme for 2018-19, and played for the winning Great Britain team at the 2019 Rugby Europe Women’s Sevens Olympic Qualifying Tournament. This later propelled your career to the height where you have been at the top of English women’s rugby. Tell us more about your professional journey of exceptional hard work, tenacity, and endurance?
I’ve always loved sport, growing up I would try anything I had the opportunity to. At primary school I was introduced to sports like tag rugby, cricket and athletics. I think being exposed to sport at a young age developed the competitive nature in me and I got so much enjoyment from it, which never went away really.
I started playing rugby because I was desperate for a new challenge, and felt like I wasn’t going to unlock my full potential in Athletics, but I said to myself I was only going to do it if I was going to play for England, I wanted to be the best, so that was in my head from the moment I picked up a rugby ball. It was a steep learning curve being thrown into an international setup with very little rugby knowledge, so that took a lot of confidence and hard work.
I picked up a lot of niggles (injuries) early on, as my body wasn’t used to the demands of the new sport, but after a year or so I was able to play freely and had a good stint being injury free. That was when I really saw my progression accelerate and I found myself playing on the world stage in front of thousands of fans in some of the biggest stadiums around the world, which are moments I will never forget.
In 2021, at the top of my game post Tokyo Olympics, I ruptured my first ACL. This was my first ‘big’ injury and it was devastating. When it happened, I remember laying on the pitch while the physio assessed me, and counting ahead 9 months (the average time it takes to return from an ACL injury) which took me to a week before our first match at the Commonwealth Games.
In that moment I knew I was going to do everything I could to get myself back for that tournament. After talks with my medical team to discuss the risks, we decided we would throw the kitchen sink at it, and against the odds, I returned to playing after 7 months and was selected for the 2022 Commonwealth Games. A dream comes true.
Unfortunately after a short 6 months back on the pitch, at the Cape Town HSBC World Series tournament, I was high tackled, and dislocated my other knee causing significant injuries including an ACL and MCL rupture and Meniscus tear. At first, my mindset was similar to my first ACL, ‘we go again’ I thought. But over time, this injury took its toll, I felt so hard done by and questioned a lot, why me? I struggled in a camp based program, to get the support I needed and wanted which affected me massively over time. I was however, extremely fortunate to have the support from external sources such as The RPA and The IRU.
After multiple scans, two surgeries, injections and countless physio and psychology sessions, I returned to playing on the HSBC World Series in February 2024 where I was able to start my journey back to loving rugby again. Still, 10 months later, I’m on that journey back to full confidence, full fitness and full enjoyment for the game, but I’m determined to get there.

It is a dream for a rugby player to play in the Olympics. You were selected as a member of the Great Britain women’s national rugby sevens team for the 2020 Summer Olympics. Tell us more about this spectacular achievement of yours?
Being an Olympian has always been my ultimate dream, it sounds silly but growing up I knew I was going to make it happen. I did think it was going to be in athletics, but life took me on a different path. A lot of rugby players actually dream of playing in a World Cup, rather than an Olympics as that has traditionally been the ‘pinnacle’. However for me, the Olympics were always my dream and it still feels strange to be able to say I’ve achieved it.
Like anything, it becomes normal over time, but it’s really lovely when people remind you of how special it really is. When you’re in the elite sport bubble, things that aren’t that normal become normal, like being an Olympian? Haha. I am so, so grateful for the coaches who took a chance on me as a 21 year old heptathlete, and in 4 years, nurtured me into a player worthy of an Olympic shirt. It really was one of the best experiences of my life.
Full Interview is Continued on Next Page
This interview is exclusive and taken by Namita Nayyar, President of womenfitness.net, and should not be reproduced, copied, or hosted in part or in full anywhere without express permission.
All Written Content Copyright © 2025 Women Fitness
Disclaimer
The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.



